Hospital onboarding took 7+ days. Every day was a hospital Mykare couldn't serve.
Mykare AI connects patients to 60+ hospitals across India for elective surgeries. But getting a new hospital live on the platform required a week of manual back-and-forth. As Mykare scaled, the onboarding queue became a growth ceiling.
The stakes
Mykare's business model depends on its hospital network. More hospitals means more cities, more procedures, more patients served. But every new hospital took 7+ days to onboard — a process driven entirely by manual ops work: emails, phone calls, WhatsApp messages, physical document handoffs.
As Mykare scaled from 30 to 60+ hospitals, the onboarding queue became a bottleneck that the ops team couldn't outrun. Each delay was a hospital sitting idle — patients who could have been served, weren't. The growth constraint wasn't sales. It was onboarding.
The problem
Hospital coordinators — typically time-poor, mobile-first admins — had no self-serve path to join the Mykare network. Every step required a Mykare ops member to intervene, creating a queue that grew faster than the team could clear it, with 60%+ of delays concentrated at the document submission phase.
What we found
I spoke with hospital coordinators and shadowed their onboarding experience in real time. I also interviewed Mykare's ops and sales teams to understand the internal workload on their side. Four things became clear:
Hospitals didn't know what was expected
Instructions arrived fragmented across email, WhatsApp, and phone calls. There was no single checklist. Coordinators were guessing what to submit next.
Ops was the bottleneck, not the hospitals
Every step required a Mykare team member to manually collect, verify, and upload information. The hospitals weren't slow — the process was.
60%+ of delays happened at document submission
Analytics showed the document collection phase was where onboardings stalled. Hospitals would submit partial information and go silent for days.
Coordinators needed something quick and resumable
Shadowing revealed hospital admins were managing multiple tasks simultaneously. The experience needed to be mobile-first, forgiving of interruption, and completable in stages.
Options considered
Option A — Hire more ops staff
RejectedTreats the symptom, not the cause. Adding headcount to a broken process scales the cost without fixing the experience. As hospital growth continues, the problem returns.
Option B — Improve the email templates and checklists
RejectedMarginally better communication doesn't remove the fundamental issue: every step still requires manual ops intervention. Drop-off at document submission would remain.
Option C — Self-serve onboarding portal
ChosenRemoves ops from the critical path entirely. Hospitals complete onboarding at their own pace, with a clear step-by-step structure, real-time progress tracking, and no waiting for a Mykare team member to respond.
The tradeoff
Self-serve onboarding removes the human touch that some hospital administrators — especially older, less digitally confident ones — relied on. We accepted this because the research showed coordinators weren't calling ops for guidance; they were calling because they had no other option. Given a clear, structured self-serve path, the preference was independence, not hand-holding.
We also reduced the number of form fields and steps significantly — removing anything that wasn't strictly required for a hospital to go live. The tradeoff: some information Mykare would previously collect upfront now arrives later. We decided this was acceptable because getting hospitals live faster was more valuable than collecting complete data slowly.
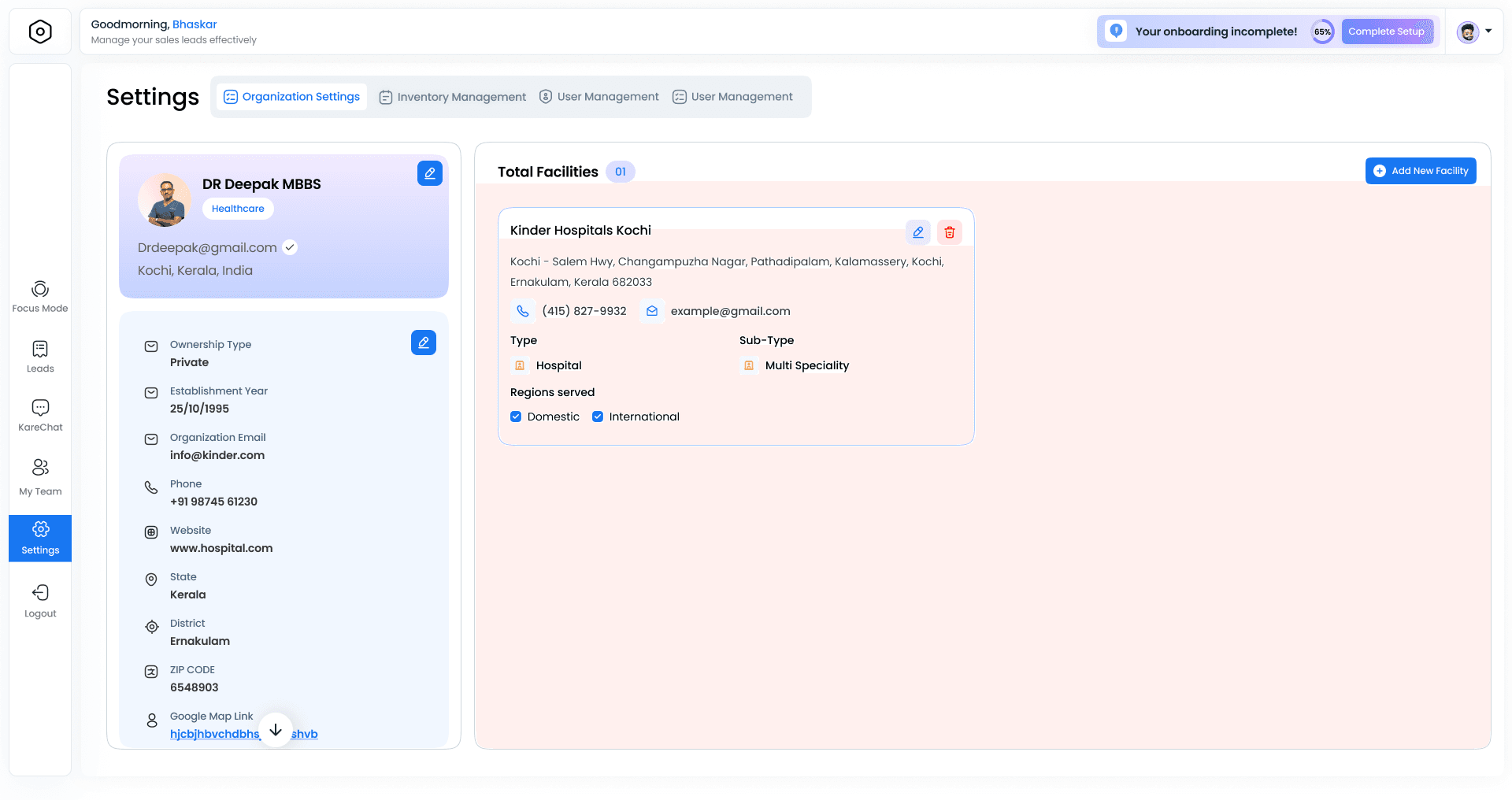
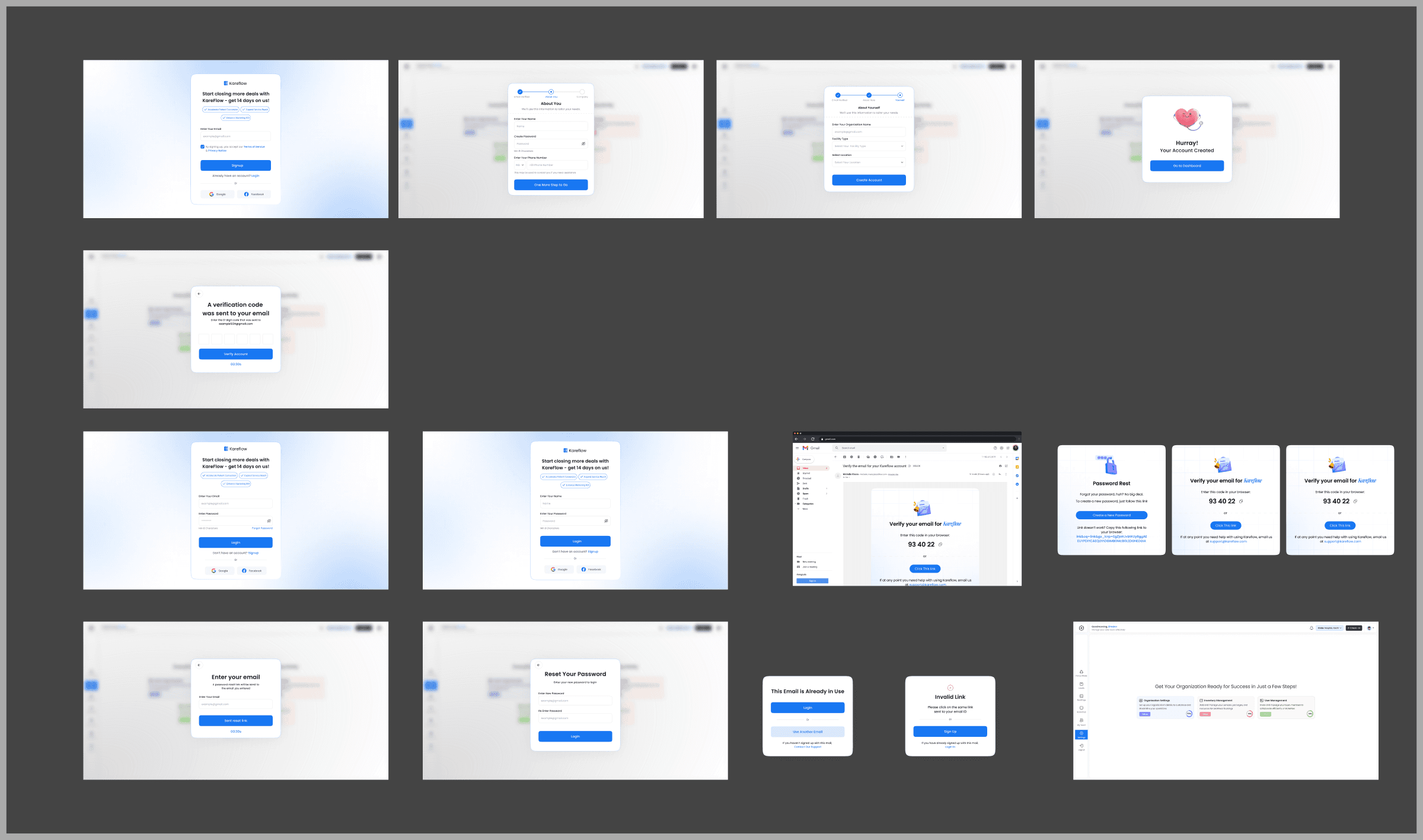
What we built
1. Step-by-step self-serve onboarding flow
A clear, sequenced onboarding journey that guides hospital admins from registration to go-live without contacting anyone at Mykare. Each step has explicit requirements, progress indicators, and the ability to save and resume — designed for coordinators who are interrupted constantly.
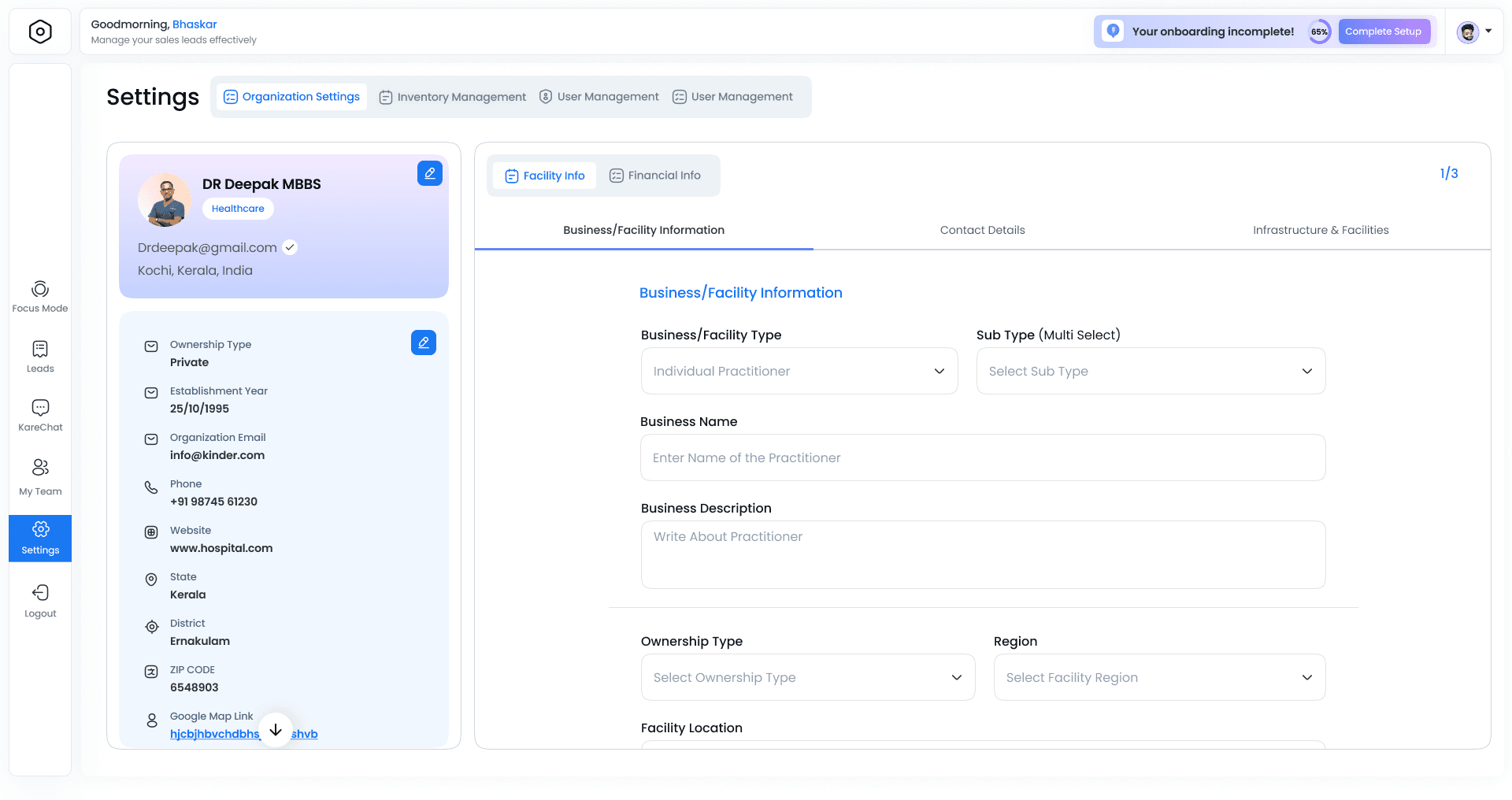
2. Restructured information architecture
The previous flow was organised around Mykare's internal ops process — not how a hospital thinks about joining a network. We rebuilt the structure around the hospital's natural mental model: who we are, what we offer, what documents we have. Every label and section header was rewritten for clarity.
3. Real-time progress tracking
Hospitals can see exactly where they are in the onboarding process, what's complete, what's pending, and what Mykare is reviewing. Eliminates the follow-up call — "just checking if you received our documents" — that previously added days to every onboarding.

Outcome
Hospital onboarding went from a 7+ day ops-heavy process to a 5–10 minute self-serve flow. The ops team — which had been a bottleneck — was freed from routine onboarding tasks entirely, able to focus on complex cases and relationship management. For Mykare, the onboarding queue stopped being a growth ceiling.
What's next
The self-serve flow handles standard onboarding well. Edge cases — hospitals with non-standard documentation, multi-location networks, specialty-specific requirements — still need ops involvement. Next: an ops dashboard that surfaces only the exceptions that need human attention, with everything routine handled by the system.